Leading through advocacy, education, and relationships
A Qualitative Study Examining the Barriers to Pancreatic Cancer Care Coordination between a High-Volume Center and Rural Physicians
Category: 2020
Author: Matthew DePuccio
Institution Affiliation: The Ohio State University College of Medicine
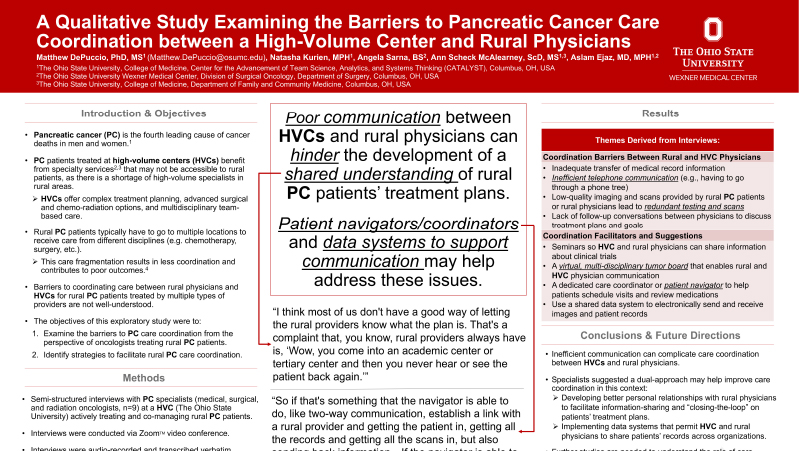
Background: Pancreatic cancer (PC) patients treated at high-volume centers (HVCs) benefit from specialty services that may not be accessible to rural patients: complex treatment planning, advanced surgical and chemo-radiation options, and multidisciplinary team-based care. As a result, rural PC patients often seek treatment at multiple locations for different episodes of care (i.e., chemotherapy and surgery). The facilitators and barriers to coordinating care between rural physicians and HVCs for rural PC patients treated by multiple providers are not well-understood. Methods: We conducted semi-structured interviews with PC specialists (medical, surgical, and radiation oncologists, n=9) at a HVC (The Ohio State University) actively treating and co-managing rural PC patients with rural physicians. Using rigorous qualitative methods, two co-authors independently coded the interview transcripts to develop a thematic account of HVC-rural physician care coordination barriers and facilitators. Results: Initial interactions between PC specialists and rural PC patients often require duplication of diagnostic testing (i.e., imaging) due to inadequate transfer of medical records at the time of consultation. This is partly due to inefficient phone communication between HVCs and rural physicians. Such inefficiencies often discourage two-way communication between HVCs and rural physicians, and this can hinder development of a shared understanding of patients’ treatment plans. Specialists suggested a dual-approach may help to improve care coordination in this context: (a) developing better personal relationships with rural physicians to facilitate information-sharing and “closing-the-loop” on patients’ treatment plans; and (b) implementing data systems that permit physicians to share patients’ records across organizations. Several specialists acknowledged the benefit of having a dedicated care coordinator who could help patients connect with specialists, navigate the different healthcare systems, and relay information between providers. Conclusions: Given the challenges that can complicate the PC treatment process for rural patients, it is important to consider opportunities to address these issues. Taking steps to improve efficiency in communication may help facilitate the development of cohesive treatment plans and promote team-based care. Further studies are needed to examine the effects of care coordination interventions, like the use of care coordinators, on improving care for rural PC patients.
Watch Video
![]() Phone: 567-712-0697
Phone: 567-712-0697
Funders & Partners
Ohio Department of Health – State Office of Rural Health
National Rural Health Association
Ohio Department of Health – State Office of Rural Health
National Rural Health Association
Find Us On


Copyright © 2026 Ohio Rural Health Association. All rights reserved.